

Calamari Clots Part 3: A Unique and Dangerous Protein Signature
Proteomics reveals a consistantly abnormal protein mixture, including abnormal fibrin structures and failure of natural clot breakdown

This is part 3 of our series examining the research trilogy by Bruce Rapley and Matt Sheldon. They investigated the strange “calamari clots,” aka “anomalous intravascular casts,” reported in both living and deceased individuals since the 2021 rollout of the COVID-19 genetic “vaccine” experiment.
Please consider supporting our ongoing work to restore human rights, uphold informed consent, and care for those who have been harmed. You can help by making a one-time donation or by becoming a paid Substack subscriber.
A special thanks to the researchers Bruce Rapley and Matt Shelton, as well as New Zealand Doctors Speaking Out with Science for sponsoring their important work.
New Zealand Doctors Speaking Out with Science (NZDSOS) is an independent group of New Zealand medical professionals advocating for scientific transparency, open debate, and evidence-based medicine. To find out more: (Click Here)
Overview of the Trilogy
In part 1, we discussed morphology and histology, which revealed consistent physical and microscopic characteristics of the casts that are completely unique when compared to all pre-existing blood clots in both living and deceased individuals. This included evidence that these structures form during active blood flow, indicating that they develop prior to death, and that they consist of dense fibrin networks with minimal cellular content.
In part 2, we examined the atomic elemental chemistry of the casts. This again revealed consistent characteristics that are completely unique compared to all preexisting blood clot types. The “calamari clots,” when compared to normal fibrinogen clots, were found to have dramatic sulfur depletion, significant phosphorus enrichment, reduced protein dominance, and other distinct and consistant features.
Now, in part 3, we will address the third study in Sheldon and Rapley’s trilogy. In this study, the researchers performed a sophisticated analysis of the casts to determine which specific proteins they contain and their relative quantities. The study is titled “Proteomic Characterisation of Anomalous Intravascular Casts Reveals Non-Canonical Fibrin Architecture and Impaired Fibrinolysis.”
In this context, “non-canonical” means abnormal and unaligned with established scientific knowledge. Part 3 represents the pinnacle of understanding so far of these strange white, rubbery casts; offering a clearer picture of their rugged structure, unrestrained growth and persistence, and the failure of fibrinolytic drugs to treat them (despite their efficacy in normal blood clots that existed prior to COVID-19 mass “vaccination”).
Scientific Method and Equipment
The researchers analyzed the protein content of the anomalous intravascular casts using the following method:
Extracting the protein: The AICs were broken down and mixed into a solution that dissolved proteins. The mixture was then centrifuged to separate out any undissolved particles, leaving only the purified protein solution


Cleaving the proteins into peptides: An enzyme called trypsin was used. Trypsin, which is also produced by your pancreas to digest protein, cleaves proteins into shorter strands by selectively cutting after the amino acids lysine or arginine. In this way, each protein was broken into peptides approximately 5 to 20 amino acids in length.

Analyzing the peptide solution: The resulting solution was analyzed to identify the extracted proteins. This involved established high-precision methods using a combined system of High Performance Liquid Chromatography and Tandem Mass Spectrometry (HPLC–MS/MS).

High Performance Liquid Chromatography and Tandem Mass Spectrometry (HPLC–MS/MS)



How This Analysis Works
In the High-Performance Liquid Chromotographer, the peptides are separated by sending them through a long, thin column one by one, separated by time. Different peptides come out at different moments. As each peptide exits the chromatograph (HPLC), it goes straight into the dual mass spectrometer. The first mass spectrometer measures the peptide’s mass, then breaks it into smaller pieces, and the second mass spectrometer measures those fragments. This creates a unique “fingerprint” that allows the computer to identify which protein the peptide came from.
The machine was run in “data-dependent acquisition mode”, which means it automatically picks the most important peptides to analyze in detail. Standard computer software matched the peptide fragments to known human proteins in a large database.
Using strict rules called “false discovery rate thresholds,” the researchers ensured reliable protein identification. This means that, at most, 1 out of every 100 identified proteins is allowed to be a wrong guess, making the results highly reliable.
Additionally, samples were processed independently across internationally distributed laboratories using harmonized protocols.
As complex as this computer-based data analysis is, the researchers followed standard, reliable protocols. The method outlined above is well established and known to be highly accurate.
Analysis Results
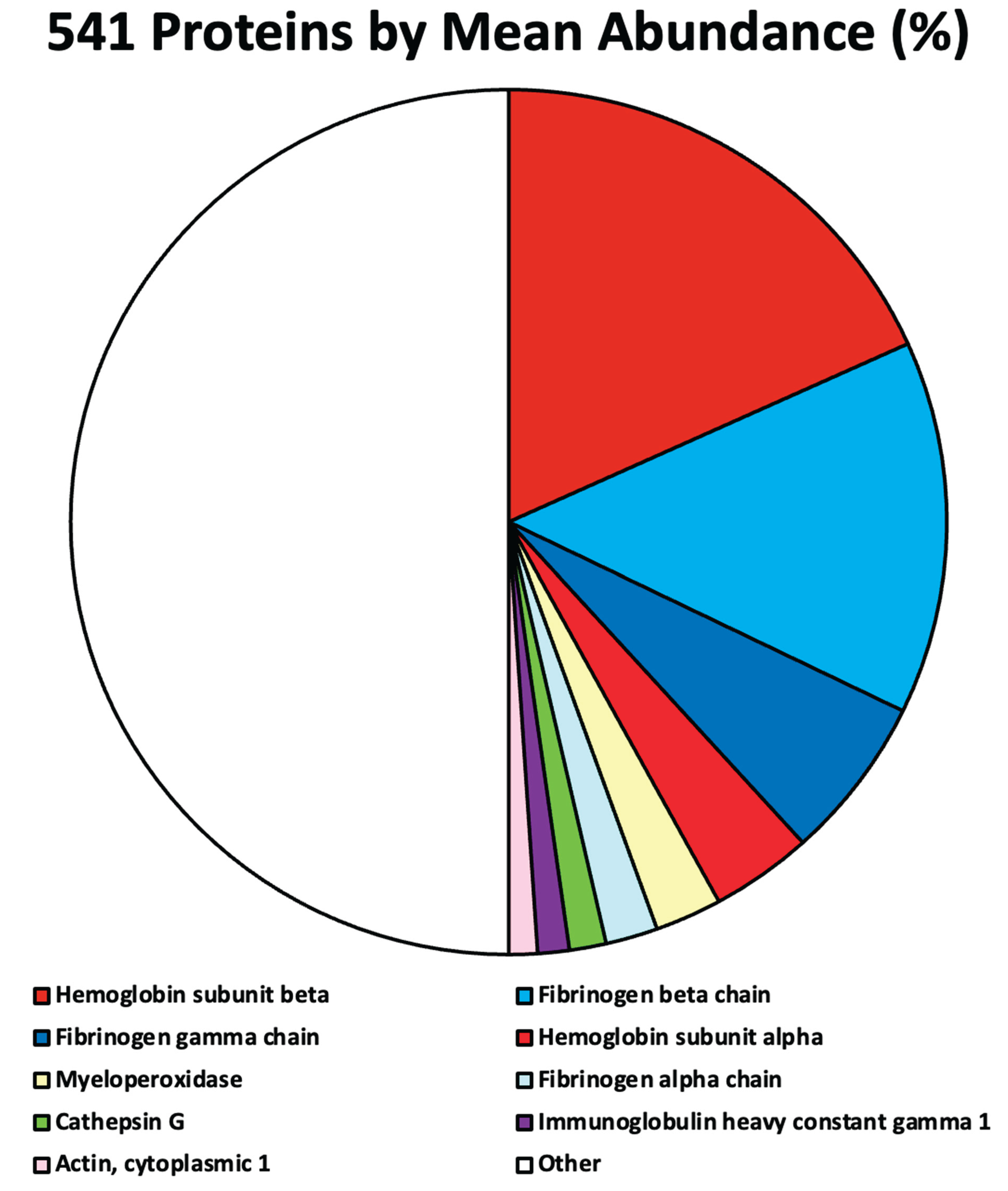
The results were consistent regardless of the sample or the laboratory. The protein content of the four anomalous intravascular casts or “calamari clots” analyzed included 541 human proteins.
532 of these proteins were present in trace amounts, so that 9 dominant proteins stood out. From highest prevalence to lowest, these 9 proteins were:
Hemoglobin subunit beta: ~17.7%
Fibrinogen beta chain: ~13.5%
Fibrinogen gamma chain: ~5.9%
Hemoglobin subunit alpha: ~3.6%
Myeloperoxidase: ~2.4%
Fibrinogen alpha chain: ~1.9%
Cathepsin G: ~1.3%
Immunoglobulin heavy constant gamma 1: ~1.1%
Actin, cytoplasmic 1: ~1.0%
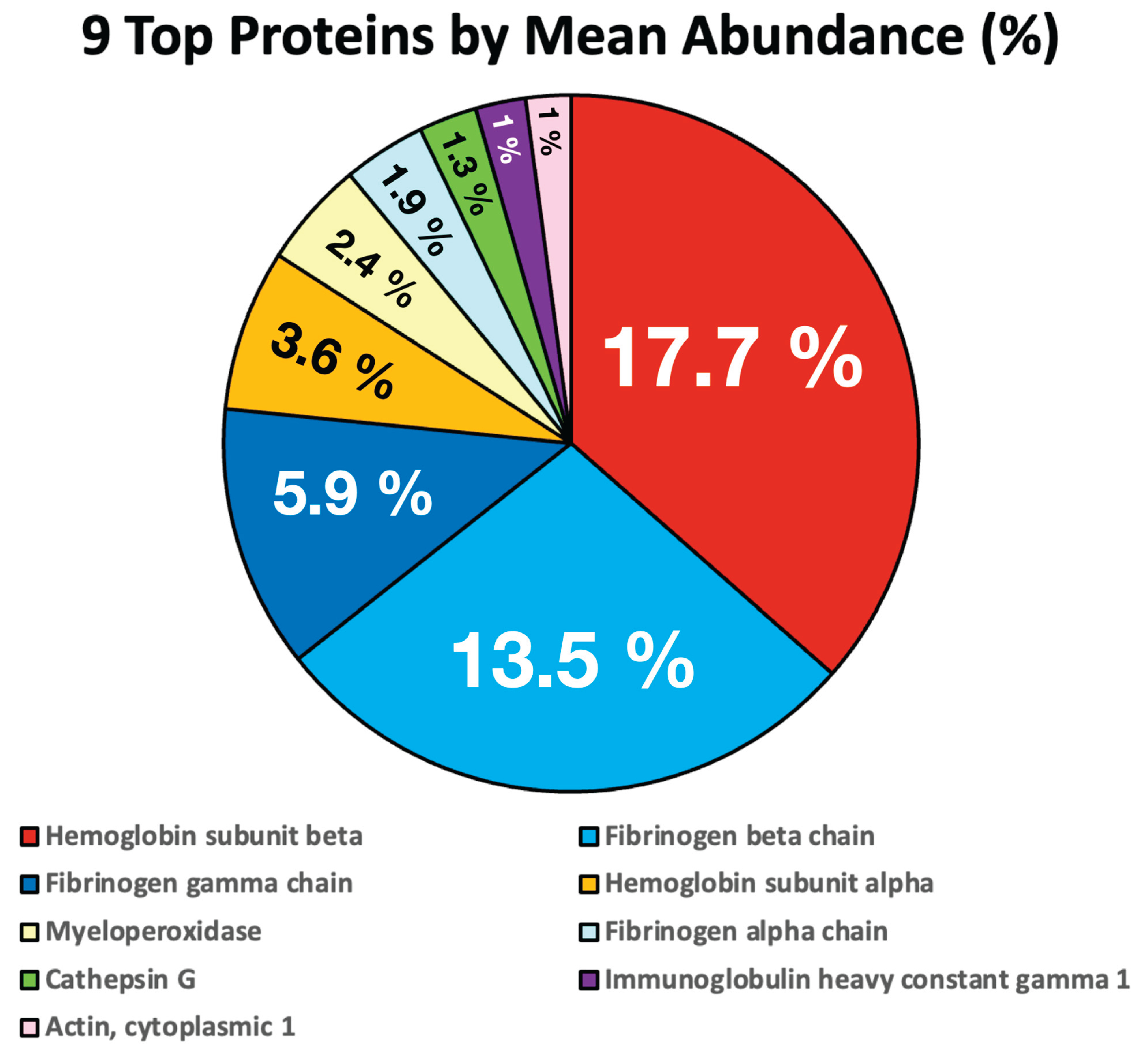
The remaining 532 proteins collectively accounted for ~48.5% of the protein content.
Discussion on the Findings
There are three key revelations that likely contribute to the calamari clots’ strong rubbery structure, unrestricted growth, persistence, and resistance to treatment:
One of the most striking findings relates to fibrinogen—the structural protein of regular bloodclots. Normal fibrinogen, is a complex protein made of three intertwined proteins referred to as “subunits” or “chains”: alpha α, beta β, and gamma γ.
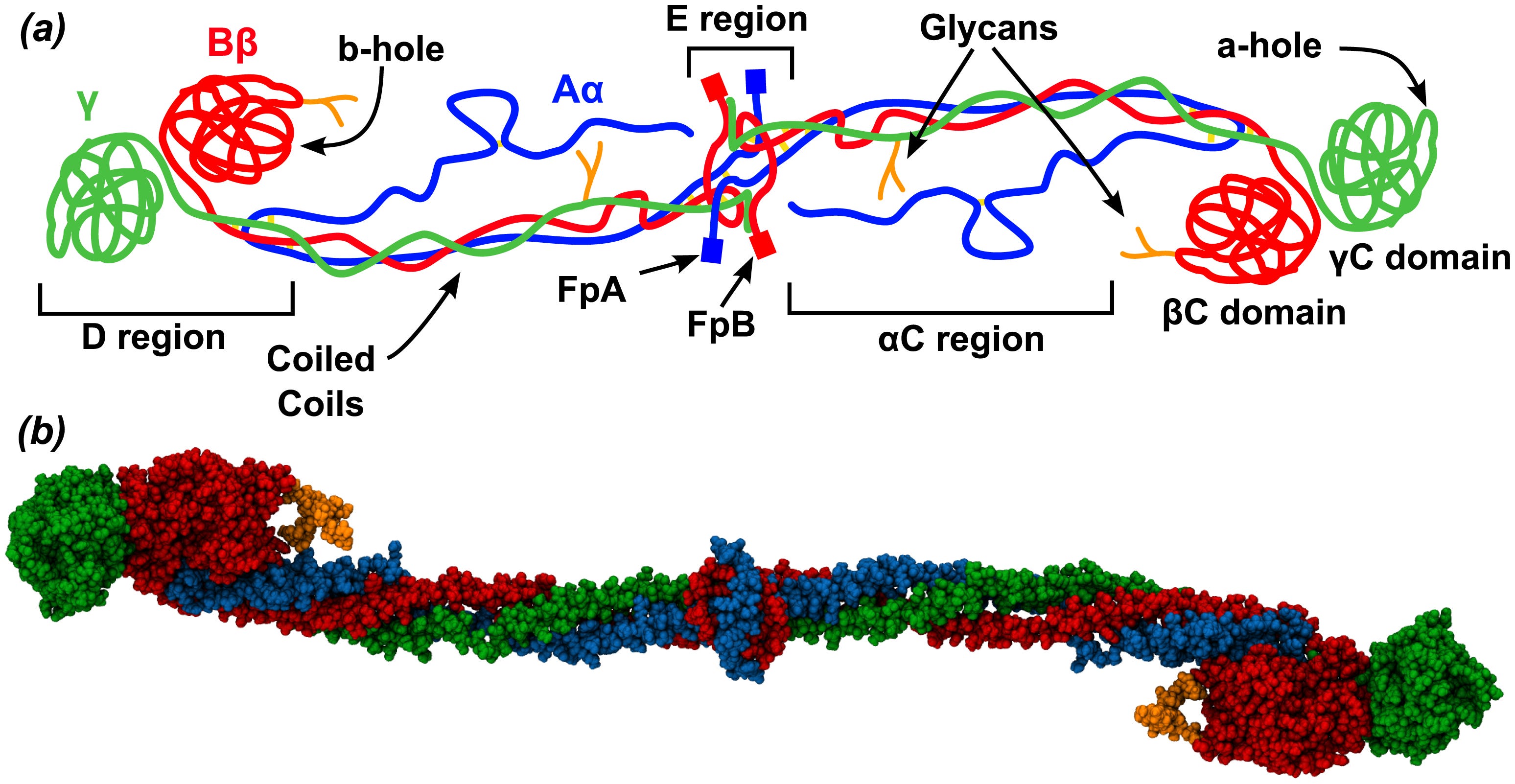
A normal blood clot composed of normal fibrinogen should have the subunits present in equal amounts, but the “calamari clots” revealed a highly abnormal ratio. Instead of the expected α:β:γ ratio of 1:1:1, these samples’ consistent ratios were α:β:γ = 1:7:3. Considering the role of fibrinogen α-chains in helping fibrinogen molecules connect in an orderly, properly spaced pattern, their relative absence is predicted to produce structures that are denser, more durable, and harder to break down. This helps explain both their strange rubbery morphology and their persistence.
Normal mechanisms, which break down clots and thus limit their size and persistence, rely on normal fibrinogen structuring. They may be ineffective for breaking down the unusual bonds of these structures. This can also help explain the failure of drugs called “fibrinolytics” in treating these abnormal “calamari clots”; fibrinolytic drugs work on normal bonds between fibrinogen molecules. This creates challenges and poor outcomes from traditional fibrinolytic treatments, which typically work in diseases involving pathological blood clotting, including: ischemic heart attacks, strokes, pulmonary emboli (blood clots in the lungs) , and venous or arterial thrombi. Since 2021, the underlying pathology in many of these medical emergencies may involve a new causative factor (the COVID-19 injections and abnormal clot structure and chemistry), meaning traditional clot-dissolving treatments are prone to failure.
Another striking finding in the “calamari clots,” which likely helps explain their durability and unfettered expansion, is a deficiency of an enzyme called plasminogen compared to normal clots. Plasminogen is an inactive protein-digesting enzyme that is normally present throughout healthy blood clots in small amounts, typically 0.3 to 0.5%. When local healing of a damaged blood vessel is complete and the clot is no longer needed, the cells lining the vessel release tPA, or “tissue plasminogen activator.” This tPA activates plasminogen into plasmin, which then works to break down the clot. In the AICs, or “calamari clots,” plasminogen was detected at only 0.13% of the total protein signal, approximately one third of its level in normal healthy blood clots.
Yet another factor that helps explain the unnatural persistence and unrestricted growth of “calamari clots” is a more profound deficiency of tPA (tissue plasminogen activator), which is needed to activate plasminogen. Of the four samples studied, three were completely absent of tPA, and only one contained tPA but in trace amounts, which were far below normal.
These three findings, fibrinogen alpha chain deficiency, plasminogen deficiency, and the absence of tPA, are all consistent with observations from funeral embalmers, clinicians, patients, and their families. The observations show that the structures grow large, resist natural breakdown, and do not respond to fibrinolytic drugs that are effective for normal clots.
Addressing the Absence of Spike Proteins
It is surprising that the researchers did not find SARS-CoV-2 spike protein within the casts. This may be explained, in part, by the fact that the analysis matched peptide fragments to a database of known human proteins; spike protein is not human in origin. Even if spike protein were present and not detected, the findings are still not consistent with the idea that these “calamari clots” are composed predominantly of spike protein.
However, we do have extensive pre-existing evidence of immune system disturbances in C-19 “vaccinated” individuals triggered by spike proteins and the random array of protein junk manufactured due to ribosome frame shifting. This is the subject of current research I am involved in and for which we greatly appreciate your donations and support.
C-19 “vaccine” induced immune system disturbances may underly the immunothrombotic findings discussed next.
Neutrophil and Immunothrombotic Involvement
The finding of the following three proteins in the structure is relevant: Myeloperoxidase ~2.4%, Cathepsin G ~1.3%, and IgG1 (Immunoglobulin heavy constant gamma 1 ~1.1%. Their presence suggests neutrophil and immunothrombotic involvement.
Myeloperoxidase, is an enzyme stored within immune cells called neutrophils. It functions within those cells to help eliminate various toxins within them. However, in inflammation and immunothrombosis (blood clotting triggered by immune dysfunction), MPO binds directly to fibrinogen, inducing unfolding and abnormal clot formation. MPO-derived oxidants modify fibrin structure, resulting in denser, thinner fibers with increased mechanical stability and profound resistance to fibrinolysis. The presence of elevated MPO in the casts suggests neutrophil-driven oxidative modification contributing to abnormal fibrin architecture. I suspect that further research may show how immune system changes, caused by COVID-19 modified mRNA “vaccines,” lead to increased myeloperoxidase in the casts.
Cathepsin G is an enzyme released by the immune system’s neutrophils in a process called “degranulation.” It has potent effects involving both platelets and fibrinogen, that increase blood clot formation. Its presence in the casts supports immunothrombotic mechanisms, where neutrophil enzymes contribute to platelet-driven, persistent clot-like structures that resist normal regulatory pathways.
IgG1 is the main working molecule of the antibody-based immune response. It actively fights infections by marking pathogens for destruction, activating complement, and helping immune cells attack invaders. IgG1 is also the dominant subclass of antibodies induced by mRNA “vaccines.” In addition to its role targeting pathogens for destruction, IgG1 also has a pathological role in “immuno-thrombosis” or “blood clotting triggered by the immune system. Its detection in the “calamari clots” points toward an antibody-mediated contribution to the abnormal clotting.
Hemoglobin
The top 9 proteins identified in the calamari clots included hemoglobin subunits, with hemoglobin’s beta unit being the number one prominent protein at ~17.7%, and its alpha unit being the fourth most common protein at 3.6%.
Hemoglobin is the highly specialized oxygen carrying molecule that is abundant in red blood cells, and specific to them. It is key to their life-sustaining role of carrying large numbers of oxygen molecules from our lungs to all the tissues in our bodies.
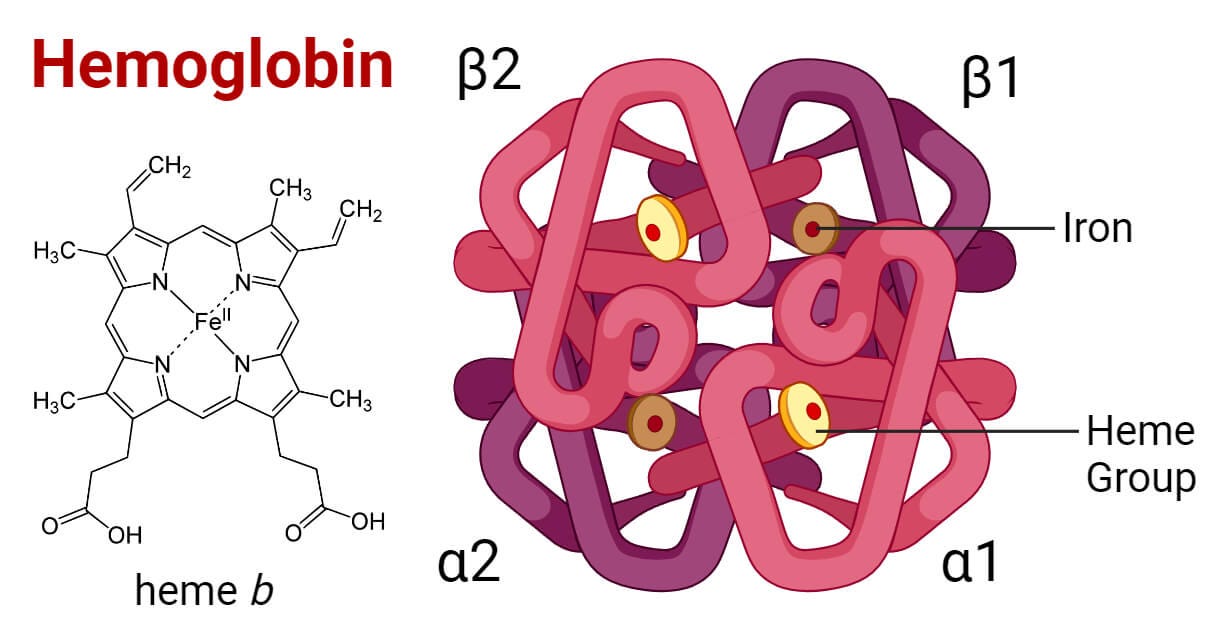
Please note that each hemoglobin molecule is constructed of two alpha and two beta protein chains or subunits. Each of the subunits contain a smaller molecule called a heme group, and each of those heme groups includes one iron atom in its structure. You may recall from the histology studies in part 1 that “intact red blood cells were largely absent. Instead, streaks of hemoglobin suggested that erythrocytes (red blood cells) had broken down within the structure.”
Also recall from elemental chemical analysis in part 2 that compared to normal fibrinogen blood clots, the “calamari clots” or AICs were high in iron, and high in phosphorus. We theorized that one possible source of this phosphorus might be cell membranes including red blood cell membranes. Red blood cells could contribute both iron from the hemoglobin heme groups, and phosphorus from the red blood cell membranes.
These findings support a process of red blood cells destruction happening concurrently with the formation of the AICs or “calamari clots,” such that red blood cell debris is captured within the forming calamari clots. Red blood cells are the only possible source of the hemoglobin protein units, a probable source of the iron, and likely contributor of phosphorus. Here, things begin to fit together.
However, the study’s protein distribution findings raise an additional question regarding hemoglobin. Why are there approximately five times as many hemoglobin beta units as alpha units, when each hemoglobin molecule contains equal numbers of both subunits, that is two alpha subunits and two beta subunits per hemoglobin molecule? This discrepancy warrants further investigation, and I will raise this question directly with the researchers. Insights or plausible explanations for the elevated beta-to-alpha ratio in these casts would be valuable information. Please share insights or theories about this, if you have them, in the comments section.
Actin, cytoplasmic 1 accounted for ~1% of the “calamari clots’” protein content. It is likely derived from white blood cells, platelets, or endothelial cells lining the blood vessels. This is also consistent with AIC formation under dynamic conditions, where blood is actively flowing and proteins can be captured as the structures form.
The remaining 532 proteins identified in the “calamari clots” were present in minute quantities. Rather than serving a specific structural role, the authors suggest these are likely background proteins in the blood that become trapped during AIC formation under flowing conditions. They also note that the deficiency of fibrinogen alpha chains likely leaves many binding sites on the remaining fibrinogen subunits exposed. These open sites may help capture and retain a wide range of other proteins within the AIC matrix as it forms.
What about spike proteins?
As previously highlighted, a anticipated finding which did not manifest in the protein analysis was the presence of SARS-CoV-2 spike protein within the casts. However, spike protein production in recipients of the SARS-CoV-2 genetic “vaccines” is known to cause significant immune system disturbances and may contribute to the immunothrombotic processes suggested by the presence of myeloperoxidase, cathepsin G, and IgG1.
Additionally, please recall in the study methods that “Standard computer software matched the peptide fragments to known human proteins in a large database.” SARS C0V2 spike protein is not a “known human protein”. Might this have masked its presence within the clots and distorted the analysis? I will reach out to the researchers and entertain this and other questions with them soon. So stay tuned for more insights.
Conclusion
The third study in Bruce Rapley and Matt Shelton’s research trilogy on anomalous intravascular casts, or “calamari clots,” reveals a consistent and entirely new protein composition, with multiple indicators pointing to the cause and nature of these structures. Abnormal ratios of fibrinogen chains, reduced plasminogen, and absent or near-absent tissue plasminogen activator help explain their dense, durable structure, unchecked growth, and resistance to breakdown, even with fibrinolytic drugs.
Hemoglobin chains were found abundantly in the AICs, correlating with earlier findings of ruptured red blood cell components captured during cast formation. The high ratio of hemoglobin beta chains to alpha chains raises important questions that remain unanswered.
Increased levels of myeloperoxidase, cathepsin G, and IgG1 point to immune system involvement in the formation of these pathological structures. Further research and corroboration with existing evidence may help clarify the role of COVID-19 spike-protein–producing-genetic-injections, a.k.a. COVID “vaccines,” in the development of “calamari clots” and the associated harm.
Other findings are consistent with structures that form during active blood flow and capture a wide variety of proteins in the process.
Thanks again to our colleagues at New Zealand Doctors Speaking Out with Science, and to researchers Bruce Rapley and Matt Shelton, for this final installment in their important research trilogy. These insights not only strengthen our call for a long-overdue halt to these dangerous genetic injections, but they also bring us closer to developing effective treatments and methods for prevention.
Soon we will publish a condensed summary of what we now know about “calamari clots”, and explore rational towards their prevention and treatment.
Thanks for subscribing, supporting, and sharing our work.
Source Material
Read the official pre-print article: (Click Here)


What an incredibly thorough series. Knowledge is light.
My cousin was unable to walk in 2023. He had clots removed from his legs and regained mobility. One year later he was diagnosed with a very aggressive form of leukemia. He dies a few weeks later. I have lost 3 cousins and one brother-in-law to cancer, and one to a heart condition, all within one year, starting July 2024. A nephew battled colon cancer (in his 30's) and four family members have had heart issues.